Summary: The incidence of obesity in Thailand is already significantly higher than in most other countries in the region, and worse is yet to come. The potential magnitude of the problem has been recognized by Thai health experts, and some small-scale or experimental remedial programs have been initiated. Those who wield the power to effect the necessary change may, however, be much slower to comprehend the significance of this burgeoning obesity crisis. Even when they do, they will invariably struggle to develop and implement an appropriate response. Failure to act quickly and decisively in addressing this issue will incur substantial social and economic costs for the Thai community.
The terms 'overweight' and 'obesity' mean "abnormal or excessive fat accumulation that presents a risk to health" 1. For adults, overweight and obesity ranges are determined by using
weight and height to calculate the 'body mass index' (BMI = weight in kilograms divided by the square of the height in meters). The World Health Organisation defines an overweight person as someone having a BMI equal to or greater than 25, and a BMI equal to or greater than 30 as being obese.
Obesity is a huge problem in many countries around the world, and Thailand ranks in the top five Asia-Pacific nations in this regard 2. In the period 2005-2007, obesity rates in Thailand increased from 10 million in 2005 to 17 million in 2007. Since then, and despite further research and some small-scale treatment programs, the incidence of obesity has only accelerated. Furthermore, these increases are now occuring across many demographic groups, and in both urban and rural areas.
With respect to childhood obesity, statistics from Thailand's Ministry of Public Health paint a troubling picture. In the past five years, the percentage of obese pre-schoolers rose from 5.8 per cent to 7.9 per cent, whilst in school-age children the obesity rate went from 5.8 per cent up to 6.7 per cent. These figures represent obesity growth rates of 36 per cent (pre-school age) and 15 per cent (school age). Among Thailand's young adults (those in the 20 to 29 age range), the obesity rate over the same period increased by 36 per cent among men and 47 per cent for women. 3
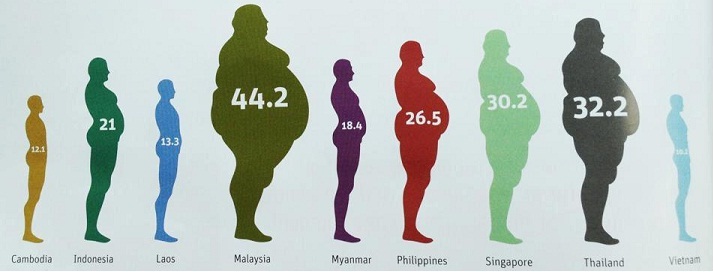
Figure One: Overweight prevalence (%) in Southeast Asia for adults of both sexes (BMI of >25kg/m2)
Source: Unknown, data drawn from WHO Non-Communicable Diseases Country Profiles, 2011
Many of the same causal factors that occur in western countries, such as poor diet, stress and sedentary lifestyle, are also present in Thailand. Here, however, additional cultural, economic and environmental factors are contributing to the problem and/or making remedial action more problematic. Indeed, the obesity epidemic now developing in Thailand has all the makings of a 'perfect storm' 4.
The shift from rural areas to the cities: This major demographic change has been occurring for some time now. Its implications include some reduction in the amount of physical activity undertaken, some weakening of family units and traditional lifestyle, and greater exposure to processed food and soft drinks.
A food-centric culture combined with a fondness for sweetness: Whilst we chit-chat about the weather, Thais routinely opt to discuss what they last ate. The Thai approach to food and eating is social and relaxed, often featuring multiple snacks or meals at irregular times of the day or night. This approach developed in a time when most ate simple foods with low calorific content, walked more, and undertook manual labour. The outcome of introducing a sedentary lifestyle and processed and high-calorie foods into this equation, was never going to be pretty. In addition, many Thai people love sweet tastes and add a considerable amount of sugar to many popular recipes. As an example, a key factor in the successful introduction of pizza to the Thai populace was the addition of extra amounts of tomato sauce (which is high in sugar) than is used in pizza topping in western countries.
The uptake of both processed food and fast food is being accelerated by 'cultural cringe': Many younger Thais are rejecting certain aspects of traditional Thai life as being decidedly 'un-cool' and old-fashioned, choosing instead to embrace available aspects of western culture/lifestyle. The implications of this include changes to earlier patterns of diet and exercise.
As in so many other countries, fast-food like KFC and McDonalds have been enthusiastically embraced in Thailand. Unlike in the West, however, fast foods are generally not cheaper or more convenient than the local fare ... demand appears to be driven more by its western cachet. Thais have not traditionally eaten things like ice cream, chocolate, and cakes/pastries. They have, however, had access to an extensive array of snack and convenience-type foods, most of which are based on staples like banana, rice, coconut, bean or tarot. Many children now however would be embarrassed to be seen with anything wrapped in a banana leaf, choosing instead products that are highly-processed, advertised on TV and wrapped in colorful foil or plastic. Further, where once water or coconut juice were seen as the beverages of choice, now flavoured (sweetened) milk and soft drinks like Coca-Cola are 'de rigeur'.5,6
Further, in selecting their recreational pursuits, many Thai children are now shunning traditional, inexpensive and accessible recreational pursuits like Muay Thai, in favor of either passive computer-based activities or more exotic and aspirational recreational activities that may often be priced beyond their reach.
A shortage of free time and disposable income: Working long hours, usually for six days each week, reduces peoples' ability and propensity to exercise. A similar situation applies with Thai children, whose school day is often drawn out with commuting and after-school tutoring. To make matters worse, most schools appear to place a low priority on sport and physical education. Little disposable income and often high levels of household debt mean that many are unable to afford to visit commercial recreation facilities such as modern gyms.
Lessening control over, and supervision of, children: The Thais love their children and like to spoil them when they are young. This trend is expected to grow as Thailand follows trends evident in many other countries, towards smaller family size, both parents in the workforce, etc. This will likely worsen the situation in terms of effective parental control over such things as diet and exercise.
A perception of chubby as healthy: This commonplace idea in Thailand that people, especially young children, are healthier and better looked-after when they are somewhat chunky, might be due to the Chinese influence whereby chubbiness equates with good luck and prosperity.
Education levels and health awareness: Many international surveys have highlighted significant deficiencies in the Thai educational environment. It is noted that, in general terms at least, more educated people are more likely to recognize the value of healthy diet and regular exercise.
A 'live for the day' outlook on life: Whilst purely conjectural, it has been suggested that Thais are more inclined to adopt a short-term outlook on life, often seemingly coupled with a poor appreciation of the concept of cause and effect. One possible implication might be greater difficulty in associating a dietary choice made today with a medical condition such as diabetes that might not manifest itself for several years.
Climate and air quality: Thailand is hot and humid for most of the year - certainly not conducive to vigorous outdoor physical activity. Dust and air pollution further discourages outdoor exercise.
Modesty and a strong focus on certain aspects of appearance: This common trait amongst Thai people has a number of implications. On the one hand, concerns about maintaining a pale appearance discourage people (esp. women) from undertaking any form of outdoor activity. Appearing tanned and/or sweaty is associated by many Thais with uncouth people. Similarly, concerns about possible body odor issues and/or the immodesty of exercise apparel act as a further disincentive to physical activity.
Poor public parks and fitness facilities: With the exception of a limited number of showpiece venues, there are few parks of adequate quality offering facilities for recreation for people of any age group. Existing facilities, such as playgrounds, are generally poorly maintained and often unsafe.
Difficult and dangerous exercise corridors: Some of the factors here include broken and uneven pavements strewn with hazards such as uncontrolled electrical wiring and signage, difficulty in safely and quickly crossing roads, dangerous driving/riding habits, the prevalence of aggressive dogs in public spaces, and the alienation of footpaths for stalls and parking.
Anticipated weaknesses in the Government's response: History suggests that the Thai Government has great difficulty in formulating and implementing programs that require multiple public agencies to coordinate their actities to achieve a shared objective. An example of this is the haphazard and woefully ineffective response to serious seasonal air pollution. Thailand's endemic system of patronage which sees myriad fiefdoms competing for privilege lies at the core of this problem. Clearly this does not bode well for issues such as obesity, where there is a clear need for many agencies and different levels of government to work side by side.
Another factor contributing to this situation are the imperative of 'face' combined with pronounced nationalism and ethno-centralism. These traits see the Thai authorities often appearing to deny or play down problems until they are impossible to ignore, usually by which time they have become entrenched and more difficult to remedy. At this point the Thai hierarchy will not wish to be seen to copy remedial programs adopted by other countries, i.e. "We are different-it won't happen to us", later followed by "We are different-we will find our own solution". Such an approach will, unfortunately, invariably lead to a delay in the implementation of an effective remedial program.
What now needs to be done?
Addressing the issue of obesity needs to be assigned a high priority, and a multi-agency Task Force should be established to:
- confirm and clarify the nature and magnitude of the current problem
- evaluate existing anti-obesity programs in Thailand as well as successful programs in other countries
- develop an actionable response, with clearly assigned lines of accountability, and
- measure and report the effectiveness of remedial action taken
To have a reasonable chance of success, such a Task Force would require adequate power, expertise, and budget, as well as a deadline by which they must produce measurable results. There should be a role for universities and hospitals, government agencies, NGO's and private companies in both developing and implementing the Task Force's strategy.
The general nature of some of the likely recommendations might include:
- Commissioning further research into cost-effective means of reducing and treating obesity
- Developing and implementing an education program aimed at all age groups, with a focus on diet and exercise, and the harmful health effects of obesity
- Improving and facilitating public access to healthy recreational opportunities, for example through:
- initiating a grants program to local government to facilitate the design, construction and maintenance of well-sited and adequate quality designed parks and recreation facilities
- initiating a program of subsidies or rebates to private service providers to provide free or reduced-cost access to recreational activities, or treatment services
(Bruce Bickerstaff is the author of 'Your Investment Guide to Thailand', which is available in hard-copy or e-book format, online and/or from select bookstores. See www.burning-bison.com for details)
References and further reading:
Last updated: 14 July 2013